Introduction to Pediatric Fractures
Fractures are common injuries in pediatric patients, often seen in the emergency department. Children’s bones are more flexible and have active growth plates, making them prone to specific fracture patterns and remodelling. Recognising fracture types, red flags and appropriate disposition is crucial for safe management.
Common Pediatric Fractures
Below are some of the most common fracture patterns in children:
| Fracture Type | Features |
|---|---|
| Greenstick Fracture | One side of the cortex is broken, while the other side is bent. Typical in younger children due to bone plasticity. |
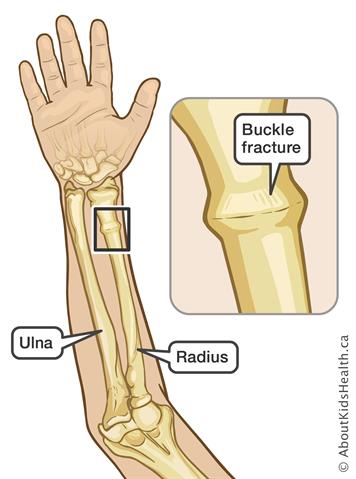
| Torus (Buckle) Fracture | Compression injury causing a bulge or buckle in the cortex. Stable, with intact periosteum. |
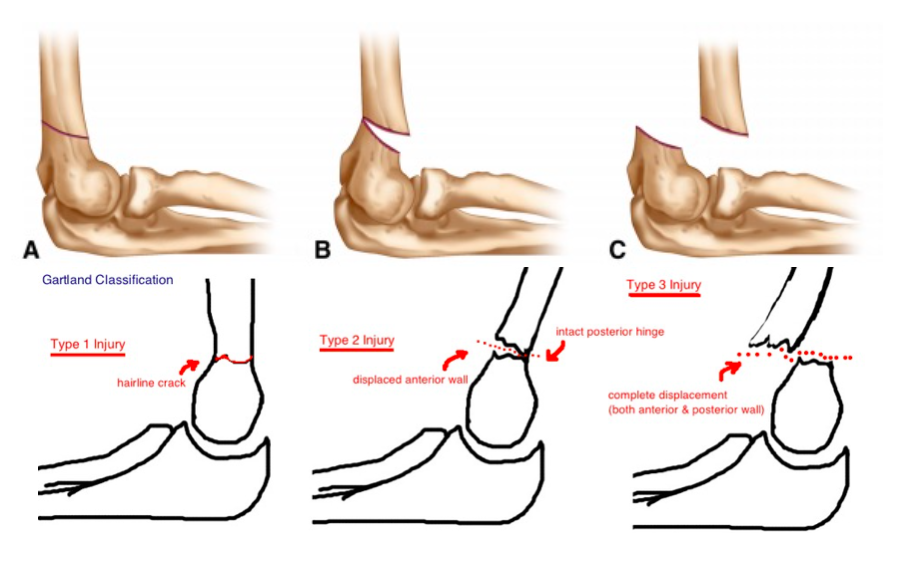
| Supracondylar Humeral Fracture | Fracture of the distal humerus just above the elbow joint. High risk of neurovascular compromise and compartment syndrome. |
| Clavicle Fracture | Common fracture of the collarbone, often after a fall on an outstretched hand or shoulder. Usually managed with a sling. |
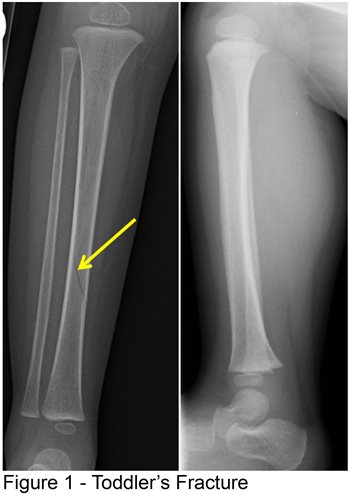
| Toddler's Fracture | Low-energy spiral fracture of the tibia in toddlers. May follow minor trauma and can be subtle on initial X-rays. |
Salter-Harris Fractures
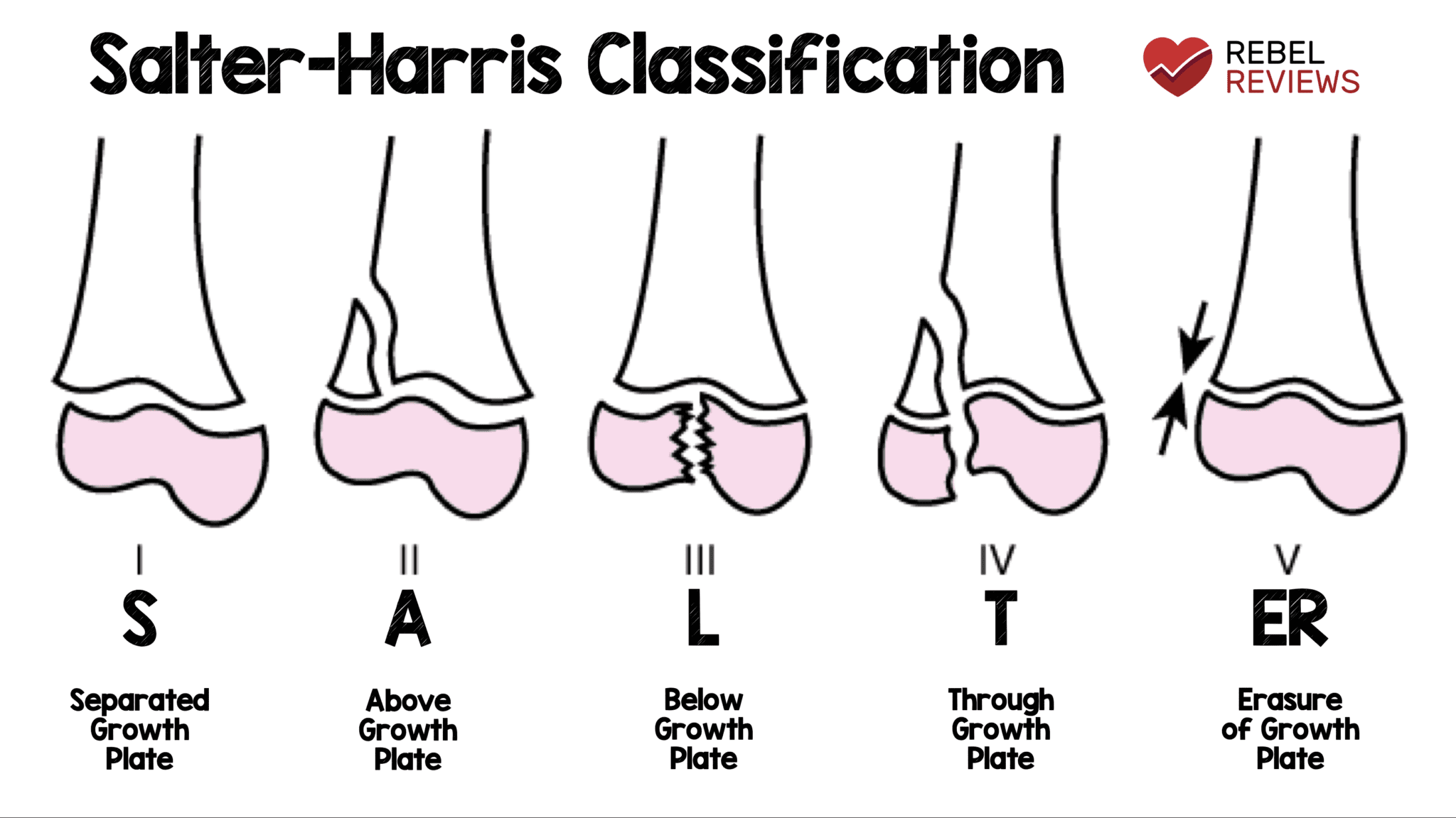
Salter-Harris fractures involve the growth plate (physis) and can impact future bone growth. Classification helps guide prognosis and management:
| Type | Description | Treatment |
|---|---|---|
| Type I | Fracture through the physis only, separating epiphysis from metaphysis. | Immobilisation; usually good prognosis. Ortho review if displaced. |
| Type II | Fracture through physis and metaphysis, sparing epiphysis. Most common type. | Closed reduction and immobilisation; orthopedic referral if significantly displaced. |
| Type III | Fracture through physis and epiphysis, involving the joint surface. | Orthopedic consultation; often needs anatomical reduction and sometimes surgery. |
| Type IV | Fracture through metaphysis, physis and epiphysis. | Urgent orthopedic consultation; usually surgical fixation to preserve the joint and growth plate. |
| Type V | Crush injury to the physis, often subtle initially on X-ray. | Orthopedic follow-up; high risk of growth arrest, long-term monitoring needed. |
Pediatric Hip and Leg Injuries
Various hip and leg injuries can affect pediatric patients. Important conditions to recognise:
| Injury | Features | Treatment |
|---|---|---|
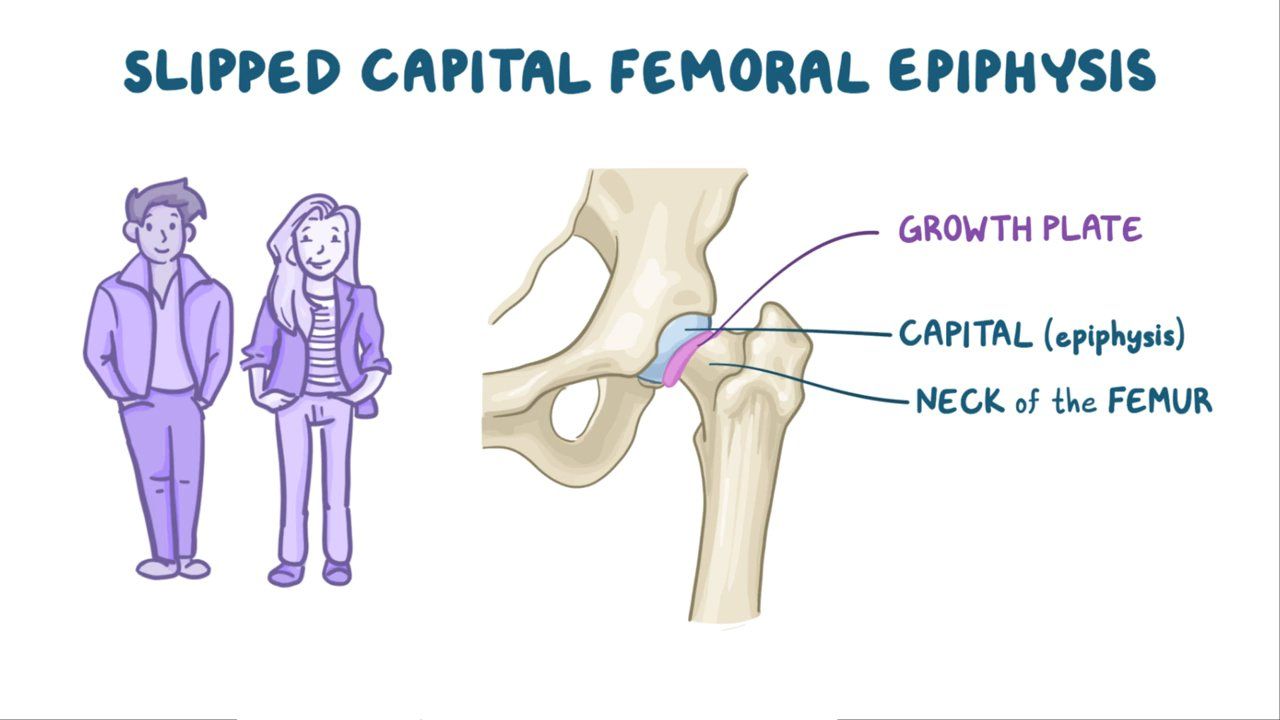
| Slipped Capital Femoral Epiphysis (SCFE) |
|
|
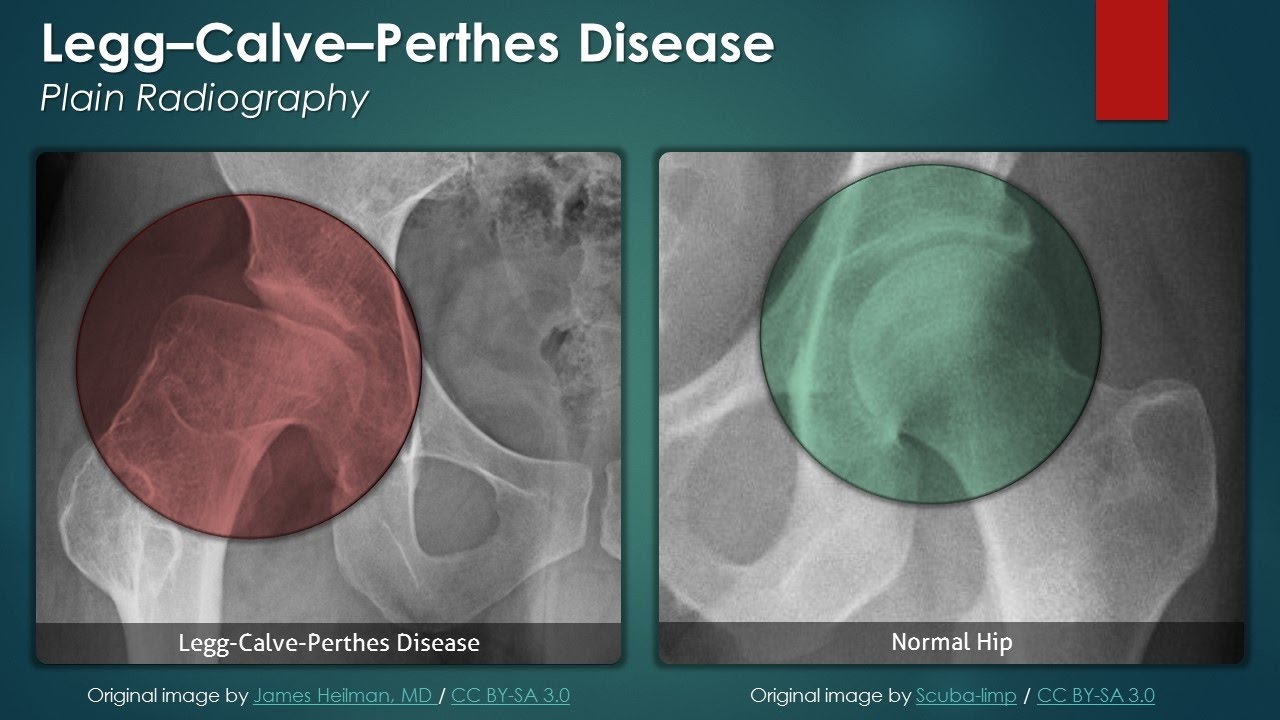
| Legg-Calvé-Perthes Disease |
|
|
| Developmental Dysplasia of the Hip (DDH) |
|
|
Pediatric Fracture Red Flags in the ED
These findings should prompt urgent senior/orthopaedic review and often admission:
- Neurovascular compromise: weak/absent distal pulses, cool limb, delayed capillary refill, sensory loss, or motor deficit.
- Severe pain out of proportion to injury, especially pain on passive stretch → think compartment syndrome.
- Tense, swollen compartments or rapidly increasing swelling.
- Open fractures or fractures with significant skin tenting or threatened skin.
- Marked displacement, angulation or dislocation involving a joint.
- Supracondylar fractures with any neurovascular abnormality.
- Multiple fractures or injuries suspicious for non-accidental injury (NAI).
- Associated head injury, polytrauma, or haemodynamic instability.
- Inability to bear weight or mobilise after lower limb injury despite adequate analgesia.
Neurovascular Assessment & Compartment Syndrome
Always document a full neurovascular examination before and after any manipulation or casting:
- Circulation: distal pulses (e.g. radial, dorsalis pedis), capillary refill time, limb temperature and colour.
- Sensation: light touch and pinprick over nerve territories (e.g. median, radial, ulnar; peroneal, tibial).
- Motor: ask the child to move fingers/toes; check key muscle groups (e.g. wrist/finger extension, ankle dorsiflexion/plantarflexion).
Compartment syndrome – think of it especially in:
- Supracondylar fractures, tibial shaft fractures, high-energy injuries, tight casts/bandages.
- Increasing pain not relieved by analgesia, pain on passive stretch, tense compartments.
- Agitation, anxiety or “pain out of proportion” in a child who cannot verbalise well.
Compartment syndrome is a surgical emergency – urgent orthopedic review and fasciotomy where indicated.
Click to Enlarge



General Disposition of Pediatric Patients with Fractures
Disposition is based on fracture type, stability, associated injuries and social/safeguarding factors:
-
Outpatient Management
Stable simple fractures (e.g. buckle fractures, undisplaced distal radius, uncomplicated clavicle fractures). Provide:- Appropriate immobilisation (sling, splint or cast).
- Analgesia plan and cast/splint care advice.
- Written safety-netting and fracture clinic/orthopaedic follow-up.
-
Short-term Observation / Day Case
Fractures requiring reduction/sedation or early monitoring (e.g. some supracondylar fractures without NV compromise). -
Admission and Possible Surgery
- Open fractures, neurovascular compromise, suspected compartment syndrome.
- Unstable or markedly displaced fractures requiring operative fixation.
- SCFE, complex pelvic or hip fractures, polytrauma.
- Concerns for non-accidental injury or unsafe home environment.
-
Follow-up Care
All pediatric fractures need follow-up to:- Confirm healing clinically and radiologically.
- Monitor growth plate function and alignment where relevant.
- Detect complications such as malunion, stiffness, or growth arrest.
A multidisciplinary approach involving orthopedics, paediatrics, physiotherapy, nursing and social services (when indicated) helps optimise outcomes.